
A Boston hospital IT director usually sees the problem before anyone else does. A storage room starts filling with retired laptops, decommissioned nursing station PCs, imaging workstations, old network gear, and a rack of servers from the last infrastructure refresh. Facilities wants the space back. Compliance wants assurance that nothing with patient data leaves the building untracked. Finance wants to know whether any of it still has value.
That pile isn’t just clutter. In a hospital, every retired device sits at the intersection of HIPAA risk, Massachusetts e-waste rules, and asset recovery. If the process is sloppy, the hospital can create a reportable data exposure, mishandle regulated electronics, and lose recoverable value on hardware that still has a secondary market.
IT Asset Disposal for Hospitals in Boston works best when it’s treated as an operational discipline, not an end-of-life errand. The organizations that do this well build a written playbook, enforce chain of custody, choose the right destruction method for each asset class, and collect documentation that stands up in an audit. They also use the program to support sustainability reporting instead of treating recycling as a black box.
The Modern Hospital's IT Disposal Challenge in Boston
Boston hospitals retire a wider mix of technology than most commercial organizations. A typical disposition project can include standard endpoints, virtual infrastructure hardware, storage arrays, thin clients, biomedical peripherals, and specialized devices that may hold or touch protected health information. Some assets are obviously sensitive. Others look harmless until someone remembers they cached credentials, logs, scans, or local exports.

In Boston, the disposal question is also shaped by Massachusetts regulation. Electronics can’t be treated like ordinary solid waste, and hospitals don’t get a practical pass just because the project is urgent. Add medical privacy requirements, internal procurement controls, and departmental ownership disputes, and what looks like a simple cleanout becomes a cross-functional compliance exercise.
Why hospital environments are harder than ordinary office cleanouts
Hospitals rarely retire equipment in neat batches. One floor may be replacing clinician laptops. Another may be shutting down a research lab. The data center team may be decommissioning storage tied to an application migration. Each stream has different custody, approval, and sanitization requirements.
The hard part isn’t identifying that old equipment has to go. The hard part is deciding, asset by asset, what happens next:
- Reuse internally: Some devices should be evaluated for reassignment before disposal.
- Sanitize and remarket: Functional hardware may still offset project costs if the process is controlled.
- Destroy media on-site: Certain assets are too sensitive to move without confirmed destruction.
- Recycle responsibly: Non-remarketable material still needs documented downstream handling.
Practical rule: If your team can’t say who owned the asset, what data it held, how it left the building, and what final disposition occurred, the process isn’t defensible.
The cost center mindset causes mistakes
Hospitals often run into trouble when they frame disposition as a hauling problem. That leads to rushed pickups, incomplete inventories, and generic recycling arrangements that don’t match healthcare risk. What works in a standard office tower doesn’t necessarily work in an environment with PHI, departmental silos, sponsor restrictions, and audit pressure.
A disciplined ITAD program changes the sequence. First classify assets. Then determine sanitization. Then manage logistics. Then document value recovery and environmental outcomes. That order matters.
For hospitals that want one provider to handle secure collection, electronics recycling, data-bearing equipment, and socially responsible end-of-life processing, Reworx Recycling’s Massachusetts electronics and ITAD services fit into that model as a practical operating option.
Navigating the Regulatory Gauntlet HIPAA and Massachusetts Rules
The legal issue for Boston hospitals isn’t whether old equipment is inconvenient. It’s whether the hospital can prove it protected data and disposed of electronics lawfully. Two frameworks drive the risk analysis. HIPAA governs how the organization protects electronic protected health information. Massachusetts environmental rules govern how electronics leave the waste stream.
HIPAA liability starts before the truck arrives
End-of-life equipment remains a security issue until data is rendered unrecoverable and the hospital can document what happened. Healthcare organizations prioritize this because the exposure is obvious. 85% prioritize data sanitization during IT asset disposal to protect PHI, and improper handling has produced cases where more than 300,000 files were recovered from used devices, according to this ITAD market report covering healthcare disposal risk.
That’s why vague assurances like “the drives were probably wiped” don’t survive scrutiny. A retired laptop from a physician office, a storage appliance from radiology, or a workstation from a nurses’ station may all carry different risk profiles, but they share one requirement. The hospital needs a disposal process that is reasonable, appropriate, repeatable, and documented.
The HIPAA Security Rule requires safeguards for ePHI. In practice, that means your disposal controls have to match the sensitivity of the data and the actual assets involved. Hospitals usually get into trouble in one of three ways:
- They underestimate local storage. Teams assume data lives only in core systems and forget about caches, exports, scans, and temporary files.
- They separate asset disposal from compliance. Operations moves faster than governance, so equipment leaves before approvals and records are complete.
- They rely on informal proof. A verbal confirmation or generic pickup receipt isn’t enough when auditors ask how specific devices were sanitized.
Massachusetts makes landfill disposal a nonstarter
Massachusetts also forces a clear operational choice. The state enforces a strict landfill ban on electronics, and non-compliance can trigger fines up to $25,000 per day, as summarized in this overview of Massachusetts healthcare disposal risk and electronics rules.
For a Boston hospital, that changes the baseline. You’re not choosing between “throw it away” and “recycle it.” The landfill route is off the table for covered electronics. The key decision is whether you’ll use a controlled ITAD process with proper data destruction and environmental handling, or create unnecessary regulatory exposure by improvising.
The combined risk is operational, financial, and reputational
A hospital can comply poorly with either side of the equation. That’s the dangerous middle ground. For example:
| Risk area | What goes wrong | Likely consequence |
|---|---|---|
| Data protection | Device leaves without verified sanitization | PHI exposure and incident response burden |
| Environmental compliance | Electronics handled outside approved process | State enforcement risk |
| Documentation | Missing serials or destruction records | Weak audit posture |
| Governance | Departments bypass central policy | Inconsistent handling across sites |
Hospitals don’t get judged on intent. They get judged on evidence.
The best compliance posture is built around proof. Proof that the asset was identified. Proof that custody never broke. Proof that the sanitization method matched the media type. Proof that the material went to the right downstream path. If any of those records are missing, the hospital is left defending assumptions.
What Boston IT leaders should do immediately
If your current process depends on ad hoc pickups, email approvals, or departmental discretion, tighten it now.
- Map every disposal pathway used across IT, facilities, biomed, research, and administration.
- Identify all data-bearing asset classes including devices that staff don’t usually think of as storage.
- Stop using generic recycling workflows for hospital equipment until compliance and custody controls are verified.
- Require documented destruction and recycling records for every disposition event.
That foundation makes the rest of the program workable. Without it, every cleanout becomes a custom compliance problem.
Developing Your Hospital's Defensible ITAD Playbook
A hospital’s ITAD policy should read like an operating document, not a recycling memo. It needs to tell your team what qualifies for disposition, who approves it, how each asset is classified, which sanitization methods are allowed, and what evidence must be retained. If those decisions are left to whoever happens to manage the cleanout, the policy isn’t doing its job.
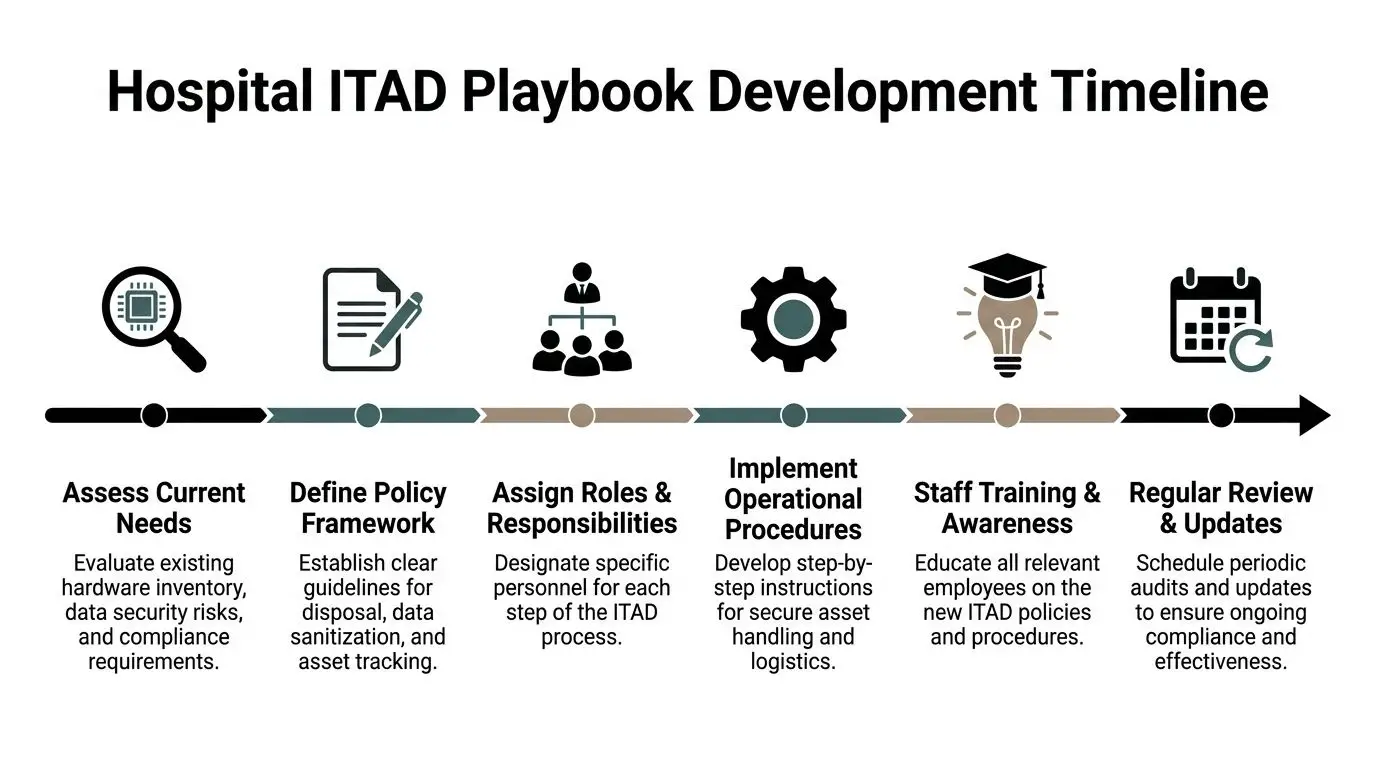
Start with a real hospital asset map
Most hospitals already have inventories. That doesn’t mean they have a disposition map. A defensible playbook begins by identifying which assets enter the ITAD stream and what makes them sensitive.
Include more than standard desktops and laptops. Pull in storage media, network appliances, mobile devices, virtual infrastructure hardware, shared department printers with drives, and medical or quasi-medical systems that may retain data. Then separate them into categories based on the disposal treatment they require.
A practical policy usually classifies assets into buckets such as:
- Data-bearing and high sensitivity
- Data-bearing and standard sensitivity
- Non-data-bearing but regulated for environmental handling
- Eligible for reuse or remarketing
- Restricted by grants, contracts, or departmental controls
That classification keeps your team from applying the same process to every device.
Assign ownership before the first pickup
ITAD failures often come from gaps between teams, not from bad intentions. IT assumes facilities is tracking the move. Facilities assumes compliance signed off. Finance assumes the vendor will report residual value. No one owns the full chain.
Build the policy around named responsibilities.
| Function | Primary responsibility |
|---|---|
| IT operations | Identify retired assets, validate technical status, coordinate decommissioning |
| Information security or compliance | Set sanitization standards and documentation requirements |
| Facilities or logistics | Control staging, access, and release conditions |
| Finance or asset management | Review remarketing, write-off, and value recovery records |
| Department managers | Confirm ownership and release approval for local devices |
This isn’t bureaucracy for its own sake. It creates a record that the hospital made deliberate decisions at each stage.
Operational advice: If a policy says “the organization” will do something, rewrite it until a specific role owns that step.
Put the policy in the same workflow as offboarding and refresh cycles
A strong policy doesn’t sit in a binder waiting for a major cleanup. It’s triggered by normal hospital events. Employee offboarding, clinic relocation, technology refreshes, data center work, mergers of departments, and research program wind-downs should all route into the same ITAD controls.
That’s where many hospitals improve quickly. They stop treating disposition as a special event and instead make it part of ordinary asset governance. Device recovery from offboarding is especially important because the easiest leaks often come from assets that disappear into local storage closets, manager offices, or home-use exceptions.
Define minimum documentation requirements
Your playbook should specify exactly what must be captured before an asset can leave control. Keep this practical and auditable. At minimum, require:
- Asset identification records such as serial number, model, and internal tag where available.
- Custody records showing who released the asset and who received it.
- Approved sanitization method tied to media type.
- Final disposition status such as reuse, resale, destruction, or recycling.
- Retention of certificates and reports for audit and legal response.
For hospitals building or revising formal procedures, this guide to implementing an IT asset disposition strategy is a useful reference point for structuring the internal framework.
Get executive approval for the trade-offs
Every hospital ITAD policy contains trade-offs. On-site destruction may reduce transport risk but can limit remarketing value on some devices. Internal reuse may support budget discipline but create more handling steps. Department-level exceptions may feel necessary, yet they weaken standardization.
Make leadership approve those trade-offs in advance. When executives sign off on the policy, the hospital avoids renegotiating basic controls every time a closet fills with retired hardware. That’s how the program becomes repeatable instead of reactive.
Executing the Disposal Process Securely and Efficiently
When the policy is sound, execution becomes much simpler. The hospital isn’t debating what to do in the moment. The team is following a controlled sequence from decommissioning to final disposition. In practice, the difference between a clean project and a messy one usually shows up in the first day of handling.
Take a common Boston scenario. A hospital is replacing aging laptops across several administrative departments, removing older servers from a secondary equipment room, and clearing out surplus peripherals from a recently consolidated clinic. The mistake would be to pile everything together and call for a bulk haul. The better move is to process the load in streams.

First control point is inventory at the point of release
Assets should be identified where they are decommissioned or at a secured staging area immediately afterward. Don’t rely on memory after the load leaves campus. Capture serials, models, and any internal identifiers that still exist. Remove or account for hospital tags according to policy, but don’t erase traceability in the process.
This is also where teams decide whether equipment is heading toward reuse, remarketing, recycling, or destruction. If that decision waits until later, chain of custody becomes weaker and reporting gets patchy.
A practical release workflow often looks like this:
- Department confirms retirement: The owner signs off that the asset is no longer needed.
- IT validates status: Systems access, configuration, and storage characteristics are reviewed.
- Asset record is created or updated: Serial and model data are captured.
- Secure staging begins: The equipment moves into locked cages, carts, or sealed containers.
- Pickup authorization is issued: Nothing leaves until the record is complete.
Choose the destruction method by media type and risk
A defensible medical equipment disposal workflow uses NIST 800-88 compliant overwriting, degaussing, or physical shredding, often on-site for sensitive assets, and on-site destruction exceeds 99% compliance in HIPAA audits according to this healthcare-focused ITAD methodology summary.
That doesn’t mean every asset should be shredded. It means the method has to fit the device and the risk.
| Method | Best fit | Main trade-off |
|---|---|---|
| NIST-aligned wiping | Reusable drives and systems suitable for remarketing | Requires validated process and logging |
| Degaussing | Magnetic media where reuse isn’t the goal | Eliminates resale potential |
| Physical shredding | Highly sensitive media or damaged devices | Maximizes destruction assurance but ends value recovery |
For many hospitals, the right answer is mixed. Standard endpoint devices with manageable risk may be wiped and evaluated for resale. Storage media from highly sensitive systems may be shredded on-site before transport of the remaining chassis.
If the hospital wants value recovery, preserve the asset where policy allows it. If the hospital wants absolute finality, destroy the media and document it.
Secure logistics are part of data security
The riskiest period is often the handoff, not the final destruction. A perfect wipe standard won’t help if devices sit in an unsecured dock or travel without custody records. Hospitals need locked containers, vetted handlers, scheduled pickup windows, and a documented transfer.
The source above also warns that skipping device recovery during employee offboarding can cause 30% to 40% of data leaks, and inadequate chain of custody contributes to 15% to 20% of non-compliance fines under Massachusetts regulations in reported benchmarks. Those are process failures, not technology failures.
For hospitals that need controlled media destruction and documented handling, secure data destruction services from Reworx Recycling align with this kind of custody-first workflow.
What usually fails in live hospital projects
The most common execution problems are easy to recognize:
- Mixed loads: Recyclable scrap, reusable equipment, and high-risk media get commingled.
- Late inventorying: Assets are counted after transport, when discrepancies are harder to resolve.
- Uncontrolled staging: Equipment waits in unsecured rooms or hallways.
- Missing offboarding recovery: Devices stay with departments or former staff too long.
- Weak paperwork: Pickup tickets exist, but no one can tie them to individual assets.
The hospitals that avoid these issues use short, repeatable checklists. They don’t rely on heroic effort from one project manager. They build the controls into each pickup and each refresh cycle.
How to Select Your ITAD Partner in Boston
Choosing an ITAD vendor for a Boston hospital is less about marketing claims and more about evidence. If a provider can’t explain how they secure media, track assets, document disposition, and support audit review, they’re not a healthcare partner. They’re a hauler with a recycling outlet.
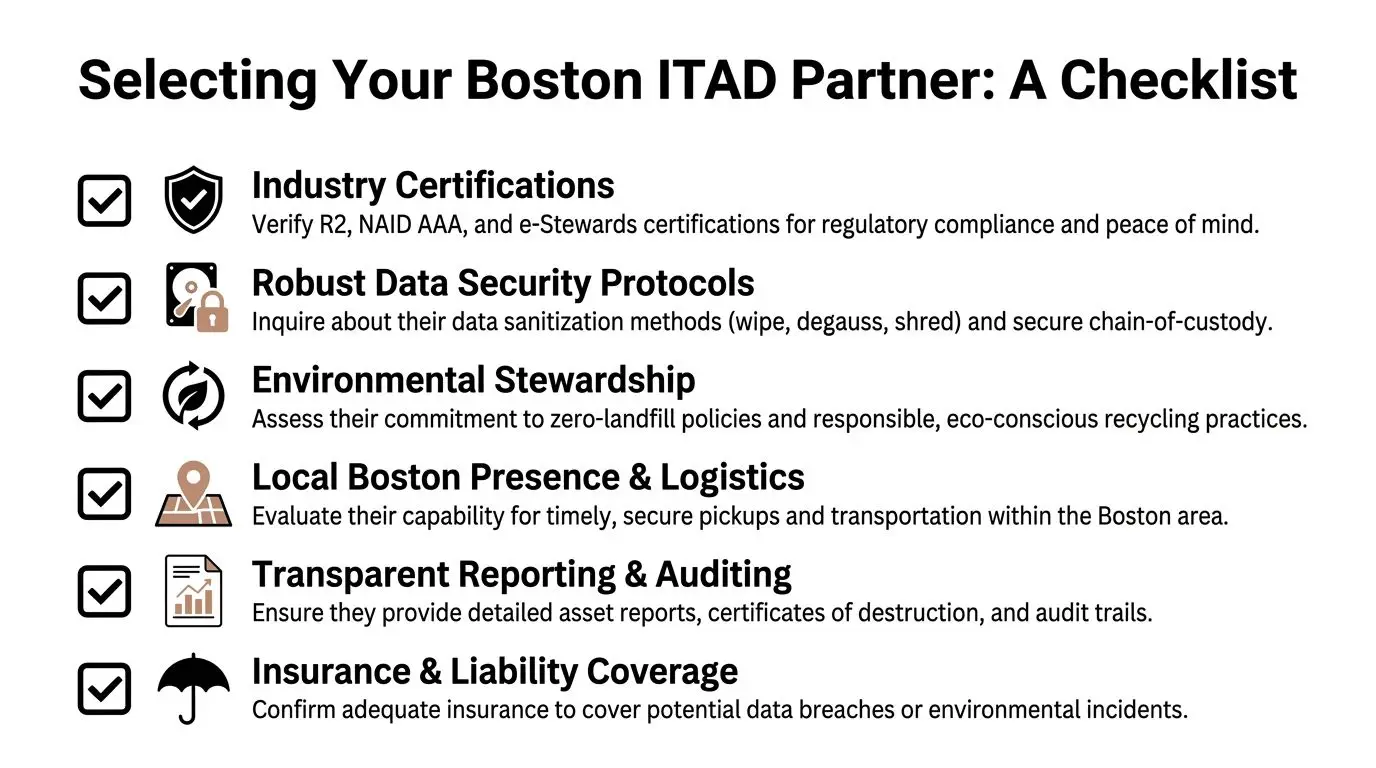
Certifications matter because they standardize proof
In healthcare, “trust us” is a weak answer. Benchmark data shows HIPAA-compliant ITAD processes achieve 98% to 100% data irrecoverability rates, R2v3 certified providers report 99.9% audit pass rates with zero verified breaches in large-scale dispositions, and in-house disposal attempts can have data recovery rates as high as 25% in forensic tests, creating healthcare breach costs in the $4 million to $6 million range, according to this Greater Boston ITAD benchmark summary. The same source notes that partnering with a NAID AAA or R2 certified firm reduces breach risks by an estimated 95%.
That’s the core reason to insist on recognized certifications. They don’t replace due diligence, but they give your hospital a defined baseline.
Questions that separate serious providers from risky ones
Use the RFP and interview process to force specificity. Ask questions that require operational answers, not polished language.
- How do you maintain chain of custody from pickup through final processing?
- Which sanitization methods do you apply to HDDs, SSDs, flash media, and embedded devices?
- When do you recommend on-site destruction instead of off-site processing?
- What asset-level reporting do you provide after pickup?
- How are certificates of destruction and recycling tied to the actual inventory?
- What happens to equipment with residual market value?
- How do you handle equipment that can’t be remarketed because media must be destroyed?
A good vendor answers these cleanly. A weak vendor drifts into generalities about being secure and environmentally friendly.
The best RFP responses read like operating procedures. The worst sound like brochure copy.
Evaluate the provider’s fit for healthcare, not just electronics recycling
A hospital should look beyond whether a vendor accepts servers, laptops, and drives. The real issue is whether they understand a healthcare environment where devices may originate from clinical departments, research spaces, admin offices, and specialty sites with different release conditions.
Use a selection checklist like this:
| What to verify | What a strong answer looks like |
|---|---|
| Data destruction capability | Clear methods, media-specific handling, documented results |
| Audit reporting | Asset-level records and usable certificates |
| Local logistics discipline | Controlled pickups, secure transport, defined handoff process |
| Value recovery | Transparent remarketing approach and settlement reporting |
| Environmental handling | Clear downstream recycling standards |
| Organizational mission | Alignment with hospital sustainability and community goals |
Hospitals that want a mission-driven option can also weigh whether the partner supports donation-based recycling and community reuse programs. That won’t replace compliance requirements, but it can support broader institutional goals around digital inclusion and responsible disposition. For vendor evaluation criteria and service scope, this overview of IT asset disposition companies is a practical reference.
Don’t outsource responsibility
Even the right vendor won’t save a hospital from a weak internal process. The hospital still owns policy, approvals, release authority, and retention of records. Vendor selection reduces risk. It doesn’t transfer accountability.
That’s why the strongest relationships are transparent. The provider shows you exactly how the work is done, where the handoffs occur, and what evidence you’ll receive. If they won’t do that during the sales process, they won’t do it after award.
Closing the Loop Value Recovery and ESG Reporting
A hospital ITAD program isn’t complete when the truck leaves or the drives are shredded. It’s complete when the hospital has the documentation to prove what happened, the financial records to account for any recovered value, and the environmental reporting needed for internal and external stakeholders.

Certificates are not paperwork clutter
Certificates of data destruction and recycling matter because they close the audit loop. They’re the records your compliance team, privacy office, legal team, and leadership may all ask for later. If the hospital can’t readily retrieve them, the disposition event remains a loose end.
Treat these records as part of the asset history. Keep them tied to inventory and disposition reports so they can be used in audit response, internal review, or litigation support. When records are scattered across email chains, hospitals waste time reconstructing events they should have documented once.
Value recovery changes the economics of disposition
Not every retired asset is scrap. Some equipment still has secondary-market value if it can be sanitized, tested, and remarketed under policy. That recovered value won’t erase compliance obligations, but it can offset refresh and cleanout costs.
The more mature hospital programs build value recovery into the front-end decision process. They don’t ask, after destruction, whether anything could have been sold. They ask before final disposition which assets should be preserved for remarketing and which must be destroyed.
For hospitals interested in that model, asset recovery programs from Reworx Recycling show how value recapture can sit alongside secure ITAD controls.
ESG reporting is where Boston hospitals can gain leverage
Boston hospitals face a practical challenge that many generic ITAD guides ignore. They need to connect secure disposal to Massachusetts-specific sustainability reporting and broader ESG expectations. That’s where ITAD can stop being viewed as a pure cost center.
A healthcare-focused sustainability reference notes that recycling 1 ton of IT equipment averts 1.5 tons of CO2, and that Mass General Brigham piloted an ITAD-linked ESG dashboard that recovered $2.1M in asset value while increasing e-waste diversion to 82%, according to this discussion of healthcare ITAD and environmental reporting in Massachusetts.
That example matters because it reframes the conversation. The hospital isn’t only paying to remove obsolete equipment. It’s producing evidence for sustainability reporting, showing diversion outcomes, and linking operational cleanup to measurable environmental benefit.
Secure disposition, value recovery, and ESG reporting work best when they’re designed as one program, not three separate tasks.
A Boston hospital that gets this right ends up with a cleaner chain of custody, better audit records, clearer sustainability reporting, and fewer unpleasant surprises during infrastructure refreshes. That’s the key outcome to aim for.
If your hospital is planning a refresh, storage room cleanout, laptop disposal project, medical equipment disposal review, or a broader IT asset disposition initiative in Boston, Reworx Recycling is one option to evaluate for secure electronics recycling, donation-based recycling, asset recovery, and compliant pickup support. If you’re mapping your next disposition cycle, start by documenting your asset classes, custody requirements, and reporting needs, then line up a partner who can support secure data destruction and sustainable recycling without forcing your team to improvise.